
Treatment Options
Findings to date suggest a potentially beneficial role for magnesium supplementation in anxiety-related premenstrual symptoms. However, methodological issues with studies limit the ability to provide definitive treatment guidelines.
Anxiety related to premenstrual stress (PMS) symptoms
Positive effects have been seen in magnesium supplementation alone, but not all studies show any benefit (1). Effects are more profound when combined with vitamin B6. It is important to note that there is a strong placebo effect in these magnesium studies which makes the evidence less reliable.
- Magnesium oxide (200 mg) combined with vitamin B6 (40-50 mg) may be effective in reducing mild anxiety related PMS symptoms (2,3)
- Doses of 200 – 500 mg magnesium oxide may have a beneficial effect on anxiety-related PMS symptoms after 2 months of daily supplementation or with supplementation over 3 menstrual cycles (4,5)
- Magnesium pyrrolidone carboxylic acid (360 mg/day) reduces subjective negative affect ratings in PMS (including tension and anxiety) after 2 months of supplementation (6)
Non-PMS anxiety treatment options
- Magnesium chloride (2000 mg, equivalent to 248 mg elemental magnesium per day) over 6 weeks improves generalised anxiety scores associated with depression (7)
- Magnesium (75 mg elemental) combined with 75 mg Crataegus oxyacantha (Hawthorn extract) and 20 mg Eschscholtzia californica (California poppy) may be effective at treating mild to moderate generalized anxiety disorder (GAD) after 90 days (8)
- Results of 2 case studies indicate that magnesium taurinate or glycinate (125-300 mg) may relieve depressive and anxiety-like symptoms in individuals suffering from major and suicidal depression (9)
- Two unpublished studies show significantly lowered somatic anxiety symptoms after 3 weeks and 6 weeks of treatment with magnesium lactate (192 mg) and vitamin B6 (20 mg). A significant placebo effect was evident in both of these studies (10)
- Magnesium oxide supplementation (200 mg/day) for 12 weeks improves quality of life ratings in individuals with mild hypertension (11)
Absorption an Bioavailability
Magnesium chloride, sulphate, citrate, lactate, malate, amino acid chelate (e.g. glycinate and taurinate) are highly biologically available whilst magnesium oxide appears to be significantly less bioavailable (12–15).
Mg-L-threonate has a higher bioavailability than the organic bound magnesium salts and can increase the magnesium concentration in the cerebrospinal fluid (16).
The bioavailability of magnesium forms should be taken into account when deciding on treatment options. However, the currently available evidence is insufficient to determine the relative efficacy of specific magnesium forms for the treatment of anxiety disorders (17).
Mechanism of Action
A number of potential mechanistic pathways have been described which may account for a relationship between magnesium and anxiety (16,17):
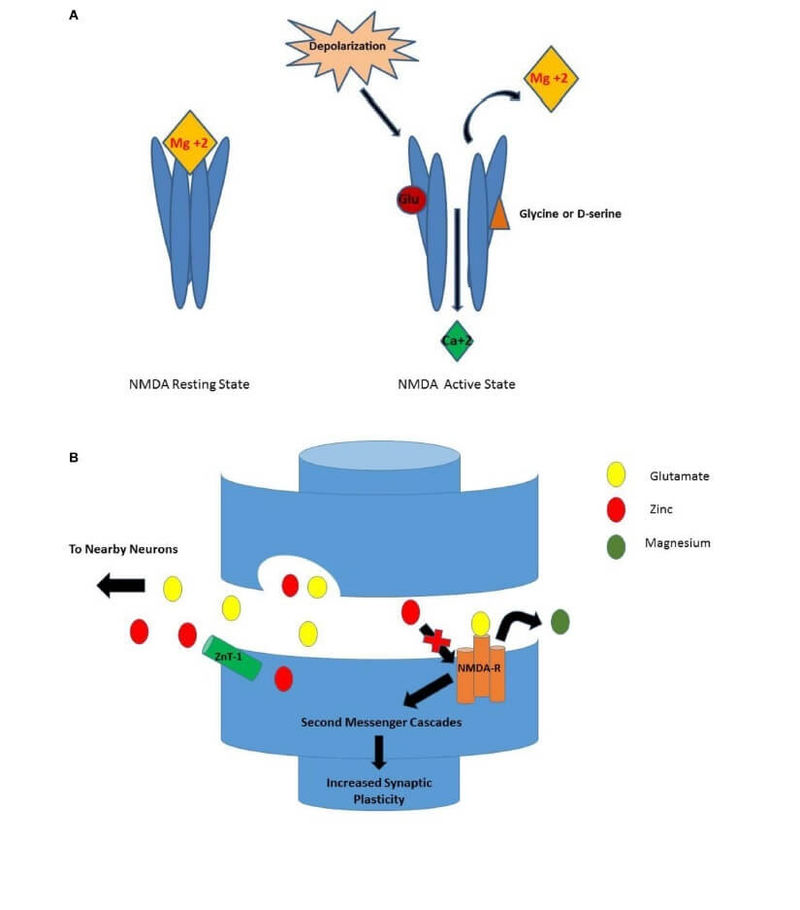
- Magnesium reduces neuronal hyperexcitability by inhibiting the NMDA receptor (Figure 1)
- Magnesium exhibits GABA receptor agonist activity by decreasing presynaptic glutamate release. GABA is an inhibitory neurotransmitter that counterbalances the excitatory action of glutamate. An imbalance between GABA and glutamate is associated with neuronal hyperexcitability characteristic of anxiety
- Magnesium is essential for the activity of mGluRs-mediated neurotransmission which is involved in the regulation of anxiety
- Magnesium may influence anxiety states via the moderation of the stress response by modulating the activity of the hypothalamic pituitary adrenal axis (HPAA)
- Stress (including anxiety) increases the need for magnesium
Figure 1. Magnesium and NMDA receptor. When Mg+2 is situated at the entrance of the calcium channel it forms a plug which blocks the NMDA receptor (18)
(A) NMDA Receptor Activation. While in the resting state, Mg+2 blocks the Ca+2 ionic pore. For a neuron to become depolarized, both glutamate and glycine must bind to their respective sites for removal of the Mg+2 ion and permit entry of Ca+2 through the pore. (B) Activation of NMDA-R as Seen in Synapse. When depolarization occurs, glutamate is released from the presynaptic terminal and binds to the NMDA receptor. Once serine binds, the Mg+2 ion is released from the ionic pore allowing Ca+2 to enter. The result is a variety of second messenger cascades that result in increased synaptic plasticity.
Foods Containing
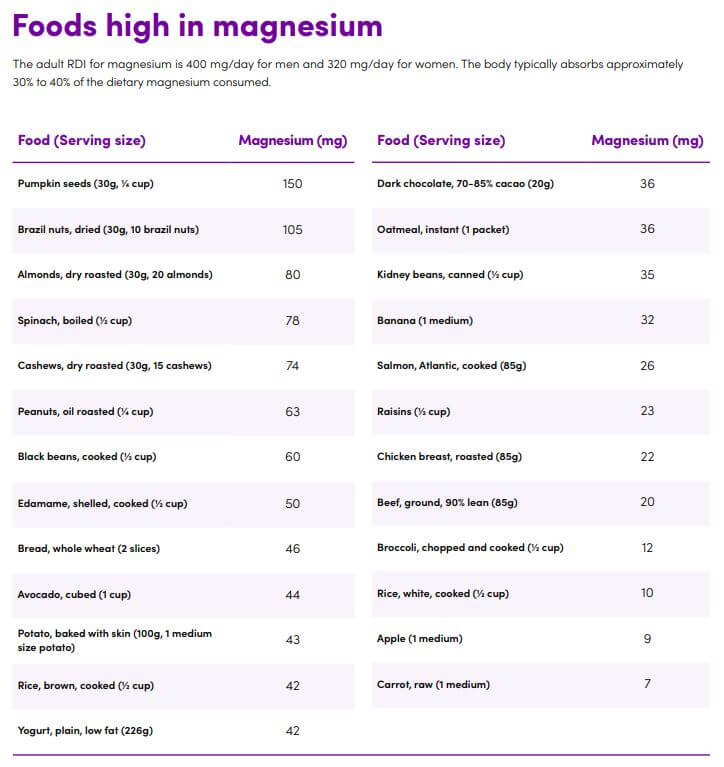
The adult RDI for magnesium is 400 mg/day for men and 320 mg/day for women (19). The body typically absorbs approximately 30% to 40% of the dietary magnesium consumed (20,21).
Table 3. Foods high in magnesium
Common Markers
Common markers used to determine magnesium status include:
- The serum magnesium concentration test is the least sensitive to magnesium status unless there is a severe magnesium deficiency
- The magnesium loading test measures urinary magnesium levels and is considered the gold standard; however, it cannot be used in individuals with kidney disease
- Ionized magnesium levels
- Red blood cell magnesium
Ionized magnesium concentrations and the magnesium loading test may be more accurate than the serum magnesium concentration (26).
Cautions/Contraindications
Magnesium supplementation is well tolerated but the following should be kept in mind (27,28):
- Magnesium salts (e.g. oxide, citrate, chloride, lactate) can cause gastrointestinal symptoms, including diarrhoea, nausea and vomiting
- Concomitant use with doxercalciferol, or with urinary excretion-reducing drugs such as glucagons, calcitonin, and potassium-sparing diuretics, may increase serum magnesium levels
- Concomitant oral intake may influence the absorption of aminoglycosides, bisphosphonates, calcium channel blockers, fluoroquinolones, skeletal muscle relaxants and tetracyclines. Avoid where possible
- Parenteral magnesium should not be given to patients with renal impairment due to the increased risk of heart block or hypermagnesemia
Takeaway on Magnesium and Anxiety
Evidence to date offers modest support for the use of magnesium in individuals with mild to moderate levels of anxiety.
The effects of magnesium on anxiety in experimental studies provide a rationale for proposing that magnesium will have a beneficial effect on mild to moderate anxiety. There are also sufficient potential mechanisms of action to support the role of magnesium in the treatment and prevention of anxiety. However, the quality of clinical studies is poor and further rigorous evidence is required.
The strongest evidence relates to magnesium supplementation in women suffering from premenstrual related anxiety, especially in combination with other ingredients, such as vitamin B6.




