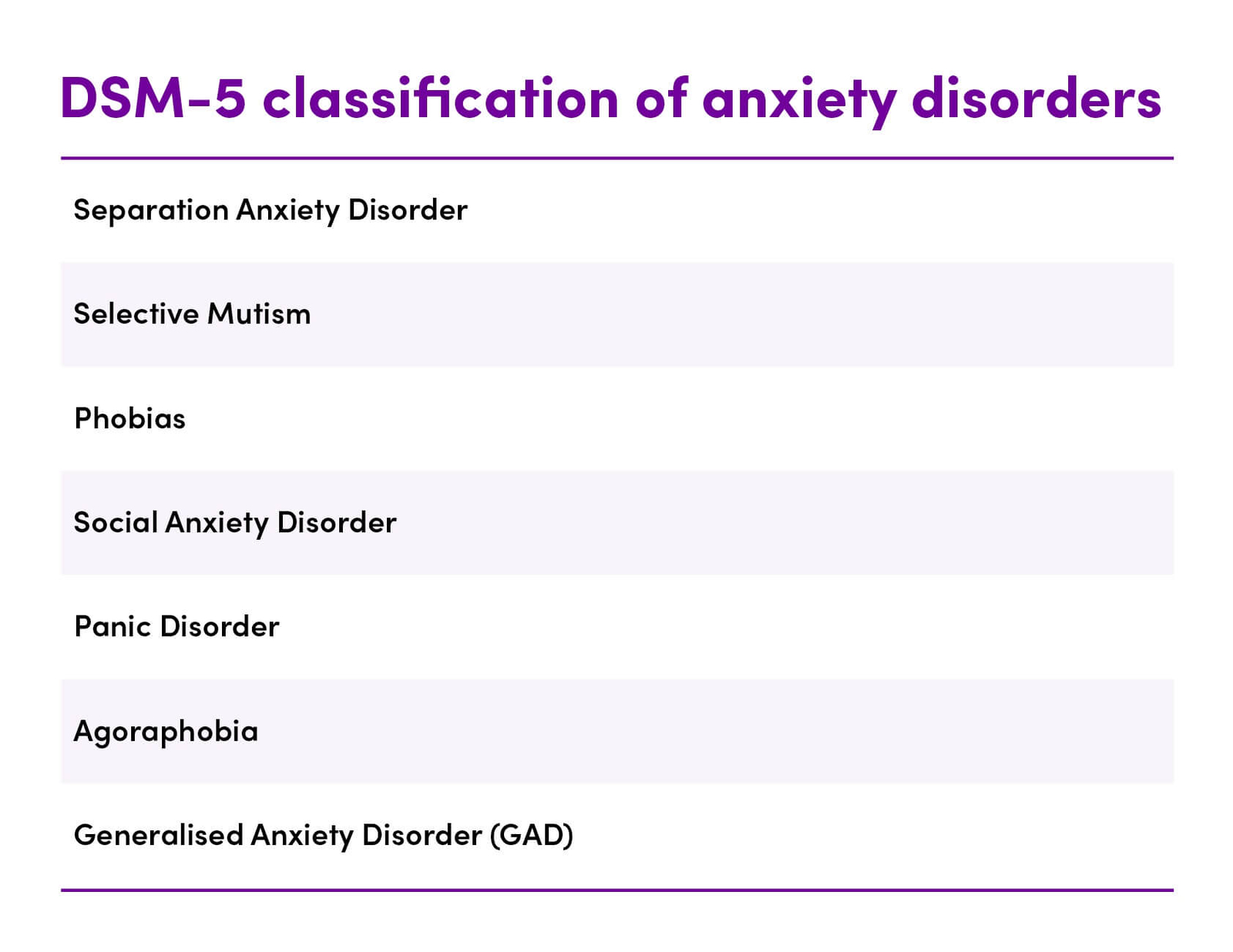
Anxiety and related disorders are among the most common of mental disorders in the general population, with one in three adults being affected during their lifetime (1,2). The Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5) identifies seven categories of anxiety disorder (Table 1).
Table 1. DSM-5 classification of anxiety disorders (3)
Anxiety is a normal human emotion which arises during stress and/or discomfort. However, if left uncontrolled, anxiety can lead to debilitating overwhelming fear with symptoms of restlessness, worry, irritability, muscle tension and sleep problems (2).
Magnesium (Mg) is an essential mineral which serves as a cofactor in more than 600 biochemical activities in the body including adrenalin and neurotransmitter synthesis and neuronal cell metabolism (4). Magnesium may play an important role in the aetiology of affective mood disorders and supplementation may be beneficial in alleviating anxiety symptoms (1).
Dietary intake of magnesium is insufficient in Western populations and one-third of Australians do not meet the intake requirements (1,5).
Traditional Understanding
Pharmaceutical anxiolytic treatments for clinical anxiety (Table 2) are often accompanied by multiple negative side-effects (1).
Table 2. Pharmaceutical antianxiety agents (2).
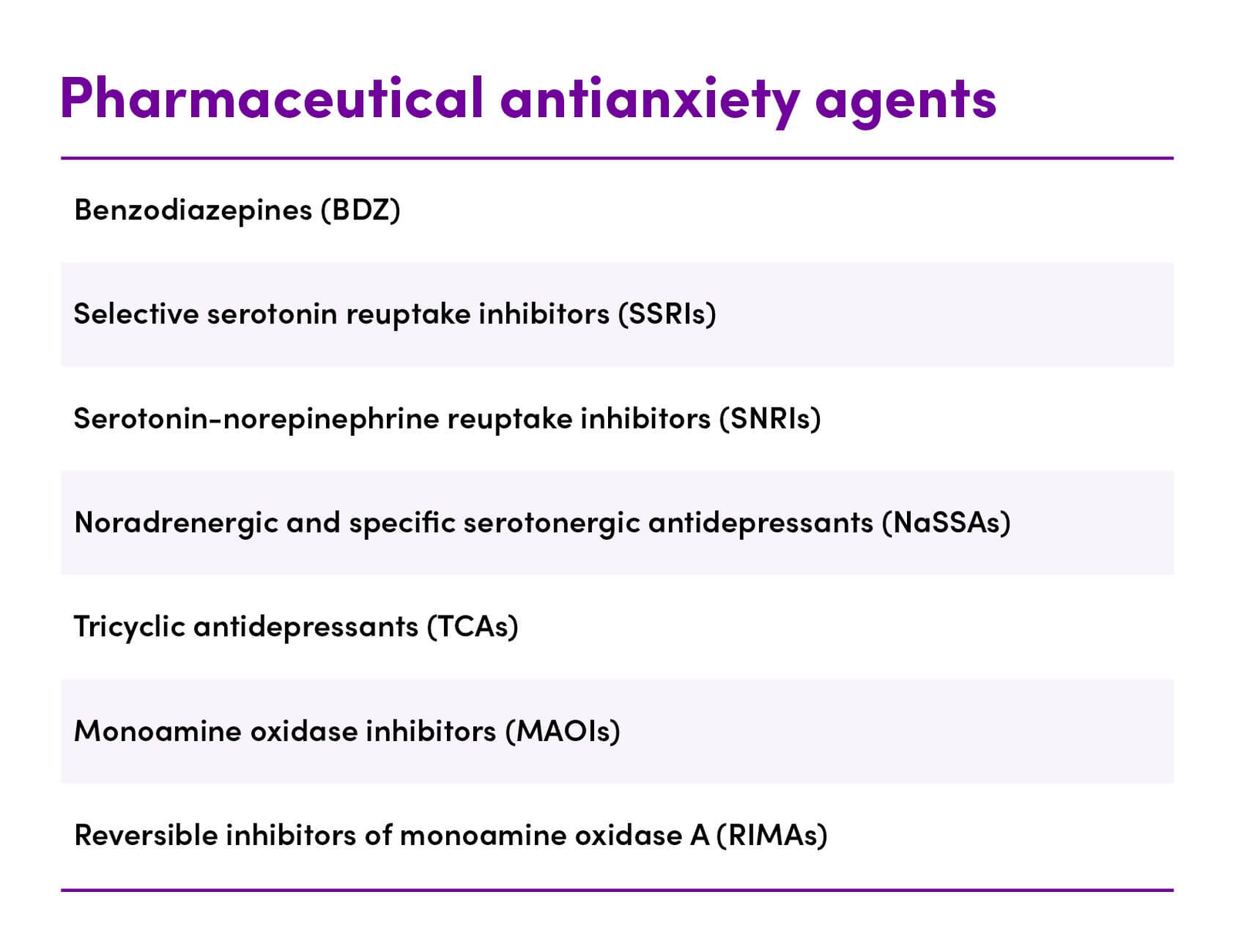
Benzodiazepines, SSRIs, SNRIs and other anxiolytics are often effective, however, there is a need for rapidly acting, better-tolerated medications with a greater and more sustained response (2).
Anxiety disorders are commonly diagnosed using mental questionnaires and by verbal consultation. Neither diagnosis nor therapy is easy and understanding the pathophysiology is crucial for accurate diagnosis (2).
Latest Research
The latest research is limited. However, studies indicate that there may be a relationship between magnesium status and anxiety.
- In individuals suffering from depression, magnesium supplementation (2000 mg magnesium chloride equivalent to 248 mg elemental magnesium) over 6 weeks resulted in an improvement in generalised anxiety scores associated with depression compared to placebo (6)
- Individuals with obsessive-compulsive disorder (OCD) have decreased serum magnesium levels compared to a control population (7)
Experimental studies
- Magnesium deficiency produces anxiety-related behaviours, an upregulated stress response and HPA axis dysregulation (8)
- A magnesium deficient diet changes the levels of gut microbiota (9,10). The absence of the gut microbiota is associated with dysregulation of stress reactivity and anxiety-like behaviour and leads to increased activity in the amygdala, the brain region critically involved in anxiety (11,12)
Limitations of Magnesium-Anxiety Research
Research to date indicates that there may be a beneficial effect of magnesium on anxiety in some population subgroups. However, the quality of the evidence is poor and includes the following limitations (1):
- Small cohort size
- Poor study design
- Lack of placebo control (important given that studies that did include a placebo found a significant placebo response)
- Lack of use of a measure of anxiety other than subjective anxiety
- Lack of data on dietary intake, including social –economic status of the cohorts, which would influence dietary intake and may bias the overall results
- Large heterogeneity in the studies (form, dosage and duration of magnesium supplementation)
- No baseline measures of habitual magnesium intake
- Lack of recording of serum magnesium levels, which might affect magnesium absorption from supplementation. Pre-trial vs post-trial comparison of serum magnesium levels would give a better understanding of absorption over a range of magnesium intakes
Pathophysiology of Magnesium Deficiency
Magnesium deficiency is not uncommon in the general population (13–17) and may be caused by:
- Decreased dietary intake, particularly in Western diets (e.g. low oxalate diet)
- Dietary deprivation (e.g. calorie restricted diets)
- Food processing (e.g. frying significantly decreases the magnesium content of green vegetables compared to boiling)
- High levels of alcohol consumption
- Poorly controlled diabetes
- Malabsorption (e.g. chronic diarrhoea, malabsorption syndrome, Crohn’s disease, coeliac disease, ulcerative colitis, intestinal resection).
- Renal disease
- Endocrine causes (e.g. hyperthyroidism, hyperaldosteronism, hypercalcaemia)
- Medication use (e.g. antibiotics, proton pump inhibitors, diuretics, chemotherapeutic agents)
- Parasitic infections (e.g. Blastocystosis)