
Nutrients interact in a synergistic manner in the body to maintain homeostasis.
Intestinal absorption and subsequent metabolism of a particular nutrient, to a certain extent, is dependent on the availability of other nutrients (1).
Magnesium and vitamin D are two essential nutrients that are necessary for the physiologic functions of various organs.
Studies have shown that the activities of three major enzymes determining 25(OH)D level (2-5) and vitamin D binding protein (3) are magnesium dependent (Figure 1) (6).
Figure 1: Magnesium and metabolism of vitamin D. Adapted from (6) CC BY 2.0
PTH, parathyroid hormone; UVB, ultraviolet B; VDBP, vitamin D binding protein
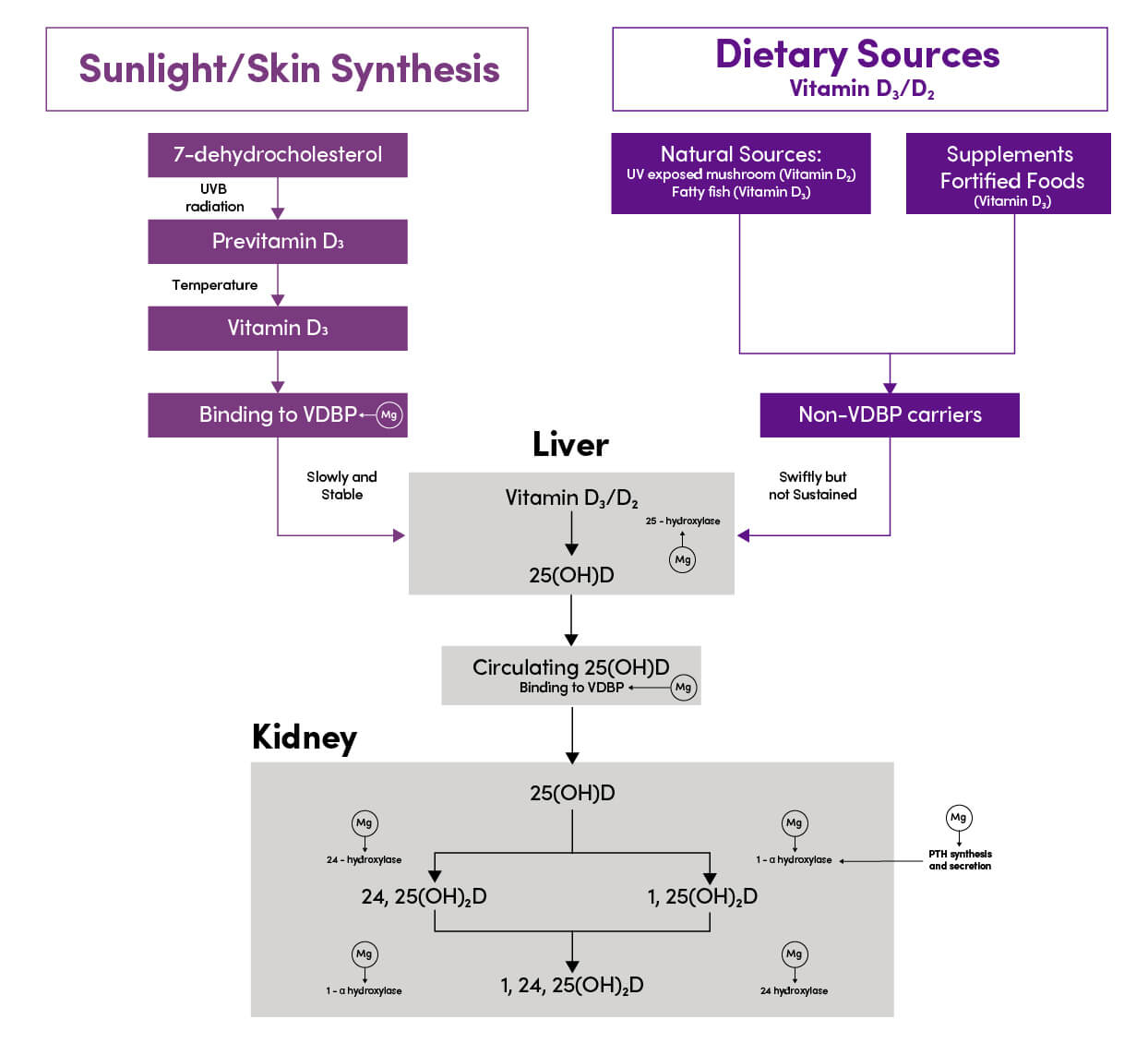
In turn, activated vitamin D (1,25(OH)2D) has been shown to stimulate intestinal absorption of magnesium (1).
A study based on the NHANES cohort found that high magnesium intake was associated with reduced risk of vitamin D deficiency or insufficiency in the general population. Researchers believe that this observation is the result of the interaction between various metabolic pathways that regulate 25(OH)D levels (6).
Research has also found that consuming the recommended daily intake (RDA) of magnesium may be more effective in preventing bone-thinning than vitamin D supplementation alone given magnesium’s relationship with potentiating vitamin D activities via possibly increasing its absorption and endogenous activation (7-10).
In previous studies, magnesium deficiency was found in 84% of postmenopausal women with osteoporosis diagnosed by low magnesium trabecular bone content and magnesium load testing (11).
The Australian Bureau of Statistics' Health Survey reveals about one in three adult Australians do not have an adequate intake of magnesium and 1 in 4 are vitamin D deficient (12).
According to the nutrient reference values for Australia and New Zealand, the recommended amount of magnesium is:
400 mg/day and 310 mg/day, respectively, for adult men and women aged 19-30 years. 420 mg/day and 320 mg/day, respectively, for men and women aged 31 and over (13).
Dysregulation in either magnesium or vitamin D can be associated with various disorders, including skeletal deformities, cardiovascular disorders, and metabolic syndrome (1).
There is a recent increase in global awareness of vitamin D deficiency and its supplementation is becoming common practice, however, magnesium deficiency remains unaddressed (14).
Screening for chronic magnesium deficiency has its limitations given a normal serum level may still be associated with moderate to severe deficiency. To date, there is no simple and accurate laboratory test to determine the total body magnesium status in humans (14).
Ensuring the recommended RDI for magnesium should be considered as an important aspect of vitamin D therapy.




